J Cardiovasc Thorac Res. 18(1):4-14.
doi: 10.34172/jcvtr.026.33487
Review Article
Comparing mitral transcatheter edge-to-edge repair and surgical intervention in mitral regurgitation: A meta-analysis
Emídio Mata Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Validation, Visualization, Writing – original draft, Writing – review & editing, , , * # 
Barbara Lage Garcia Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Validation, Visualization, Writing – original draft, Writing – review & editing, , #
Margarida Castro Data curation, Formal analysis, Investigation, Project administration, Validation, Visualization, Writing – original draft, Writing – review & editing,
Mariana Tinoco Validation, Visualization, Writing – review & editing,
Luísa Pinheiro Resources, Visualization, Writing – review & editing,
João Português Resources, Visualization, Writing – review & editing,
Francisco Ferreira Resources, Visualization, Writing – review & editing,
Lucy Calvo Supervision, Writing – review & editing,
Sílvia Ribeiro Supervision, Writing – review & editing,
António Lourenço Supervision, Writing – review & editing,
Author information:
Cardiology Department, Unidade Local de Saúde de Alto Ave, Guimarães, Portugal
#These authors contributed equally to this work.
Abstract
Surgery remains the standard treatment for severe mitral valve regurgitation (MR), but growing evidence highlights the potential role of mitral valve percutaneous edge-to-edge repair (M-TEER). This meta-analysis aims to compare 12-month all-cause mortality between M-TEER and surgical intervention (SMVI). A systematic search (October 2024) of PubMed, Cochrane, Scopus, and Web of Science identified randomized control trials (RCTs) and propensity-matched observational studies comparing 12-month all-cause mortality in MR patients treated with M-TEER or SMVI. An inverse variance random-effects meta-analysis assessed outcomes using risk ratios (RR) and 95% confidence intervals (CI). Two RCTs (MATTERHORN and EVEREST II) and three observational studies totaling 1,782 patients, were included in the final analysis. A non-significant trend of higher mortality at 30 days was observed in the SMVI group (RR: 0.72; CI: 0.26–2.00), along with higher complication rates mainly due to bleeding. At 12 months follow-up, SMVI was associated with a significantly lower risk of all-cause mortality (RR: 1.41; CI: 1.11–1.81), while the M-TEER group had more patients with MR grade 3 or higher (RR: 4.05; CI: 1.54–10.67), with a non-significant trend of higher rate of MR reintervention (RR 2.51; CI 0.83–7.66) at 12 months. Based on current evidence, M-TEER should continue to be reserved for patients with prohibitive high surgical risk. While propensity-matched cohorts were pooled for the study estimates, the limited available data from randomized trials, combined with heterogeneity in patient populations, particularly regarding MR etiology, underscores the need for further studies.
Keywords: Mitral valve insufficiency, Mitral regurgitation, Mitral transcatheter edge-to-edge repair, Percutaneous mitral valve repair, Surgical mitral valve repair, Mitral valve replacement
Copyright and License Information
© 2026 The Author(s).
This is an open access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Funding Statement
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Introduction
Mitral valve regurgitation (MR) is among the most common valve disorders, affecting approximately 2% of the global population worldwide.1 It occurs equally in males and females and increases in prevalence with age. MR is classified as either primary MR (PMR), caused by structural abnormalities in the leaflets, chordae or papillary muscles; or as secondary MR (SMR), resulting from left ventricular (LV) wall motion abnormalities or remodeling, without intrinsic valve defects.1
Patients with PMR usually have preserved left ventricular ejection fraction (LVEF) and generally lower surgical risks, though some may have reduced LVEF, and thus face worst surgical outcomes.2 In contrast, SMR is often associated with heart failure (HF) in about 30% of patients, with a higher surgical risk.3
While surgical intervention is the standard approach for severe MR, advancements have led to the development of mitral valve transcatheter edge-to-edge repair (M-TEER) as a less invasive option for high-risk patients.
The EVEREST II trial marked a landmark as the first randomized controlled trial (RCT) to compare long-term mortality M-TEER with surgical mitral valve intervention (SMVI) in patients with clinically significant mitral regurgitation who were eligible for surgery.4 The study revealed that M-TEER offered a superior safety profile while showing no significant differences in 12-month mortality when compared to SMVI.
Recently, a new RCT, the MATTERHORN trial,5 provided new insights, comparing M-TEER and surgical mitral valve repair in patients with SMR, concluding that M-TEER was not significantly different to SMVI regarding major adverse events at 12 months.
This systematic review with meta-analysis aims to compare mortality and immediate safety outcomes of patients with significant MR undergoing either M-TEER or SMVI by pooling results from these RCTs while also incorporating data from propensity score-matched studies to enrich the pooled population.
Methods
Search Strategy and Selection Criteria
This study was designed following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement,6 and registered on PROSPERO (CRD42024611622).
On October 11, 2024, a systematic search from inception PubMed, Cochrane Central Register of Controlled Trials, Scopus and Web of Science was conducted. The search encompassed broad terms referring to “transcatheter mitral valve repair”, “mitral valve surgery” and “mitral regurgitation” (Full query in Supplementary Material Table 1). The references’ lists of the included studies and relevant reviews were searched for additional publications. Eligible studies satisfied the following inclusion criteria: (1) RCT or observational studies with propensity matched cohorts that enrolled (2) patients with significant MR (3) undergoing either M-TEER or SMVI (4) and comparing all-cause mortality at 12 months of both groups, expressed as odds ratio, freedom from outcome or risk ratio. Single arm studies were excluded. No restrictions were applied for publication status or publication language.
Selection Process
Two reviewers independently screened all titles and abstracts for potential eligibility after duplicate records were removed. To ensure sensitivity at the abstract-level selection, full texts were retrieved in all cases of unclear abstracts or disagreement between reviewers. Full texts of potentially eligible studies were then retrieved and assessed independently by the same two reviewers to determine inclusion based on the predefined criteria described above. Discrepancies at the full-text level were resolved through discussion with a third reviewer. No automation tools were used in any phase of the screening process. All references were managed using EndNote X9 (Clarivate Analytics).
Data Extraction and Outcomes of Interest
Two reviewers independently extracted data from each eligible study, using a standardized data extraction form with information regarding study and patient characteristics, MR etiology, medical or device therapy at baseline, pre-procedure echocardiographic features, and outcomes at 30 days and 12 months.
All-cause mortality at 12 months was the main outcome of interest. Secondary outcomes were all-cause mortality at 30 days, short-term complications, New York Heart Association (NYHA) functional classification, MR grade and mitral valve (MV) reintervention at 12 months.
Risk of Bias
The risk of bias was conducted using the Cochrane risk of bias tool for RCTs and for Non-randomized Studies - Interventions, Version 2 (ROBINS-I V2 TOOL). The presence of publication bias could not be performed because only five studies were included.
Synthesis Methods
A narrative synthesis approach was primarily employed to describe and interpret findings across studies, particularly when analysis was limited due to heterogeneity in study designs, outcome reporting, populations, or outcome definitions. Structured tables grouped by intervention (M-TEER vs. SMVI) were used to present baseline characteristics, clinical outcomes, and risk of bias assessments in a standardized format to facilitate meaningful comparison across studies.
Where outcomes were sufficiently homogeneous, a study-level meta-analysis was conducted following an intention-to-treat approach. Outcomes such as all-cause mortality and MV reintervention were treated as cumulative events and analyzed using event rates at defined time points. In contrast, outcomes such as NYHA functional class and MR grade were assessed using cross-sectional prevalence at specific time points, with the number of patients still under follow-up at that time used as the denominator. For observational studies that reported only event proportions without time-to-event data, the baseline cohort size was used as the denominator unless censoring or loss to follow-up was explicitly addressed. All estimates were calculated using a random-effects model based on the DerSimonian and Laird method via Review Manager version 5.4, The Cochrane Collaboration. The effect measure was expressed as risk ratios (RR) with 95% confidence intervals (CI), analyzed using the generic inverse variance method. Heterogeneity was tested and quantified using Chi-squared test and I2 statistics. Thresholds of I2 statistic of 25% (low), 50% (moderate) and 75% (high) were defined. The statistical level of significance was two-tailed P-value < 0.05.
Results
Search Results
The literature search (Figure 1) identified 1482 articles after duplicate removal. Of these, 12 records regarding a total of five studies were included for final analysis. Of the five studies included, two were RCTs: the recently published MATTERHORN trial, 5 and the EVEREST II trial,4 represented by eight records with three publications reporting outcomes at different follow-ups.4,7,8 The remaining three were observational studies.9-11
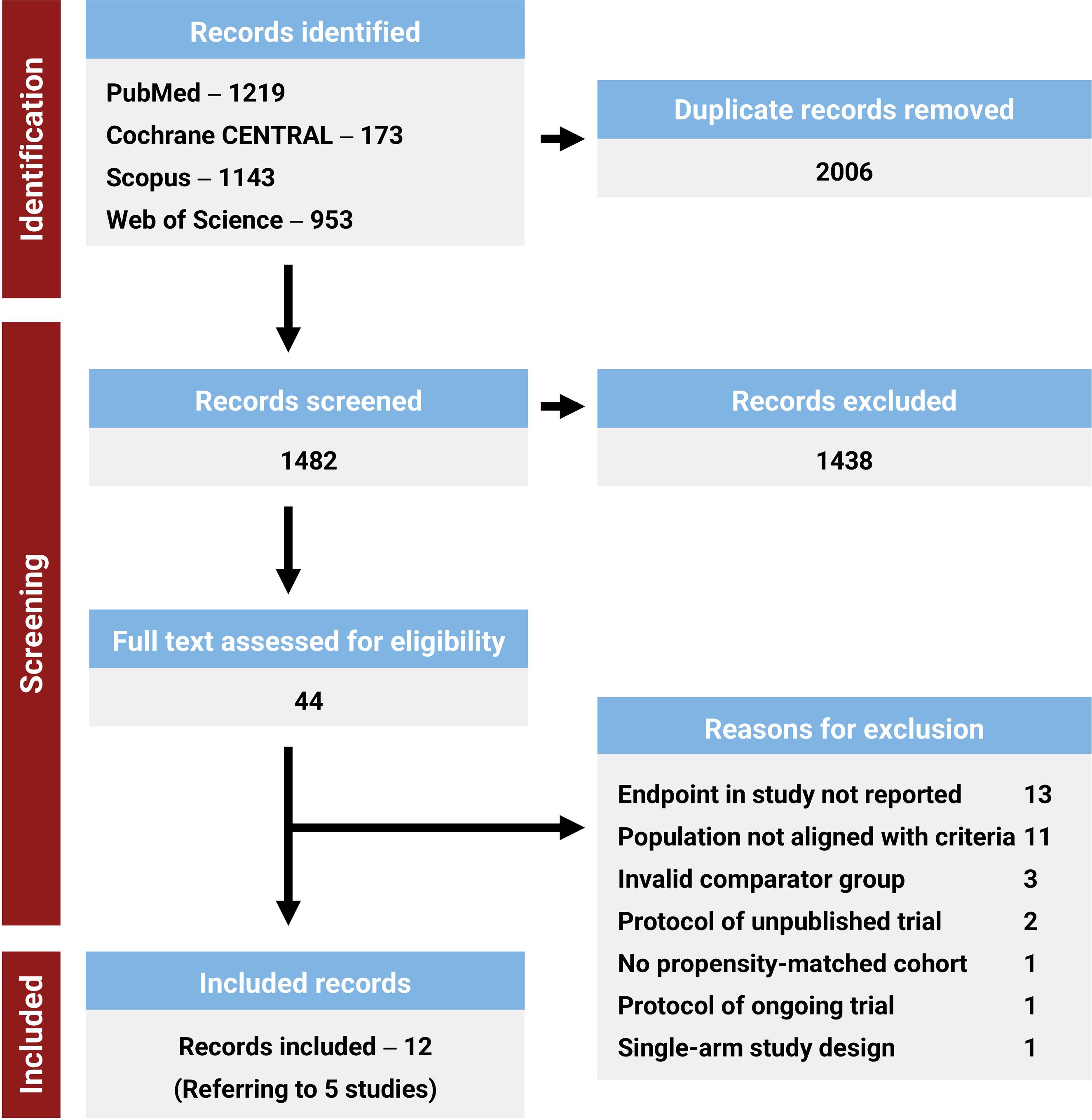
Figure 1.
PRISMA Flowchart.Study identification and selection process through the different stages of the systematic review. Cochrane CENTRAL: Cochrane Central Register of Controlled Trials
.
PRISMA Flowchart.Study identification and selection process through the different stages of the systematic review. Cochrane CENTRAL: Cochrane Central Register of Controlled Trials
Characteristics of Included Studies
Characteristics of the included studies are shown in Table 1. They were published between 2011 and 2024, across North America and Europe.
Table 1.
Included studies characteristics
Study,
Study type,
Country,
No. of centers, Recruitment Period
|
Inclusion/Exclusion criteria,
Propensity match variables
|
Number of patients
|
Mitral valve regurgitation etiology (%)
|
Surgical repair (%)
|
|
M-TEER group
|
Surgery group
|
|
M-TEER
|
Surgery
|
PMR
|
SMR
|
PMR
|
SMR
|
EVEREST II,
2011
RCT
Canada, USA
37 centers
Sep 2005 to Nov 2008
|
Inclusion criteria:
simple
-
− Moderate to severe PMR or SMR
(EROA ≥ 0.3 cm2; regurgitant volume ≥ 45 ml; regurgitation fraction ≥ 40%; vena contracta ≥ 0.5cm)
simple
-
− Eligible for both M-TEER and surgery
-
− Symptomatic: LVEF > 25% or LVESDD ≤ 55 mm
-
− Asymptomatic: LVEF 25-60% or LVESDD ≥ 40 mm, or new-onset AF, or PHT
Exclusions criteria:
simple
-
− Need for other cardiac surgery
-
− Myocardial infarction in the prior 12 weeks; endocarditis; rheumatic heart disease; serum creatinine > 2.5 mg/dl
-
− Mitral valve mitral valve area < 4 cm2, leaflet flail width ≥ 15 mm and gap ≥ 10 mm, leaflet tethering/coaptation depth > 11 mm and length < 2 mm.
|
184 |
95 |
135/184 (73.4) |
49/184 (26.6) |
69/95 (72.6) |
26/95 (27.4) |
69/80 (86.3) |
MATTERHORN,
2024
RCT
Germany
16 centers
Feb 2015 to Dec 2022
|
Inclusion criteria:
(At least 2 of: EROA ≥ 20 mm2; regurgitant volume ≥ 30 ml; regurgitant fraction ≥ 50%; vena contracta width > 8 mm) or 2 HHF in the 12 months prior
simple
-
− Eligible for both M-TEER and surgery
-
− LVEF ≥ 20% and NYHA class II to class IV
Exclusion criteria:
simple
-
− Additional severe valvular disease
-
− Coronary revascularization or CRT therapy within 1 month prior
|
104 |
104 |
0/104 (0.0) |
104/104 (100) |
0/104 (0.0) |
104/104 (100) |
72/100 (72.0) |
Koschutnik,
2022
Observational
Austria
1 center
Jul 2017 to Apr 2020
|
Inclusion criteria:
simple
-
− Moderate to severe PMR or SMR
Propensity match variables: age; EuroSCORE-II; LVEF; serum NT-proBNP levels
|
51 |
51 |
20/51 (39.2) |
31/51 (60.8) |
43/51 (84.3) |
8/51 (15.7) |
34/51 (66.7) |
Amabile,
2023
Observational
USA
58 centers
Jan 2015 to Dec 2020
|
Inclusion criteria:
simple
-
− Significant ischemic MR requiring intervention
Exclusion criteria:
simple
-
− Rheumatic heart disease; non-ischemic MR etiology; periprocedural period with acute myocardial infarction or papillary muscle rupture
-
− Patients who underwent MV replacement via surgery or through catheter
Propensity match variables: 29 variables (demographics; comorbidities; surgical history; use of CV, anti-platelet and anticoagulant medications; b-type natriuretic peptide; LVEF)
|
550 |
550 |
0/550 (0.0) |
550/550 (100) |
0/550 (0.0) |
550/550 (100) |
550/550 (100.0) |
Silaschi,
2024
Observational
Germany
1 center
Jan 2010 to Dec 2021
|
Inclusion criteria:
simple
-
− Moderate to severe PMR or SMR requiring intervention
Exclusion criteria:
simple
-
− Surgical procedures via median sternotomy; patients with endocarditis
Propensity match variables: age; EuroSCORE-II; LVEF
|
49 |
49 |
40/49 (81.6) |
9/49 (18.4) |
40/49 (81.6) |
9/49 (18.4) |
48/49 (98.0)* |
AF: atrial fibrillation; CRT: cardiac resynchronization therapy; CV: cardiovascular; EROA: effective regurgitant orifice area; HHF: hospitalization related to heart failure; LVEF: left ventricle ejection fraction; LVESDD: left ventricle end-systolic diameter dimension; MR: mitral valve regurgitation; M-TEER: Mitral valve transcatheter edge-to-edge repair; NYHA: New York Heart Association; PHT: pulmonary hypertension; PMR: primary mitral regurgitation; RCT: randomized controlled trial; SMR: secondary mitral regurgitation. * Minimally invasive surgery repair.
EVEREST II,4 conducted in 37 North American centers (2005–2008), enrolled patients with moderate-to-severe PMR or SMR eligible for both procedures, excluding those with recent myocardial infarction, endocarditis, or unfavorable valve anatomy. MATTERHORN,5 conducted in 16 German centers (2015–2022), included symptomatic patients with significant SMR, excluding additional severe valvular disease, recent revascularization or LVEF less than 20%.
Among the observational studies, two were prospectively recruited and retrospectively analyzed,9,10 while one was purely retrospective.11 Koschutnik and Silaschi focused on patients with PMR or SMR using matched cohorts based on age, EuroSCORE-II, and LVEF, while Koschutnik also including NT-proBNP levels. Amabile, utilizing the TriNetX database across 58 U.S. centers, employed International Classification of Diseases, Tenth Revision (ICD-10) and Current Procedural Terminology (CPT) codes to identify patients with SMR by selecting those with MR and ischemic heart disease.
The five studies collectively recruited 1787 patients (347 with PMR and 1440 with SMR), of whom 938 underwent M-TEER and 849 underwent SMVI (82.1% receiving MV repair). All studies focused on MV repair, with one excluding patients who underwent MV replacement,11 and another exclusively including minimally invasive surgery.9 Details of the percutaneous and surgical techniques and devices are provided in Supplementary Material Table 2.
The quality assessment, summarized in Supplementary Material Tables 3 and 4, indicated that the studies were of overall good quality.
Baseline Characteristics of the Patients
The baseline characteristics of the study population are summarized in Table 2. Male patients predominated in both the M-TEER and SMVI groups (63.2% and 61.7%, respectively), with a comparable mean age (71.3 ± 10.6 vs. 71.1 ± 9.6 years). Patients undergoing M-TEER had a slightly higher EuroScore-II risk profile (3.83 ± 3.79% vs. 3.23 ± 2.72%).
Table 2.
Study population characteristics
|
|
Age, years (n)
|
Male (%)
|
EuroSCORE II, % (n)
|
Previous cardiac surgery (%)
|
NYHA class≥III (%)
|
MR grade≥3 (%)
|
EROA, mm
2
(n)
|
LVEF, % (n)
|
LVEDV, mL (n)
|
|
M-TEER
|
Surgery
|
M-TEER
|
Surgery
|
M-TEER
|
Surgery
|
M-TEER
|
Surgery
|
M-TEER
|
Surgery
|
M-TEER
|
Surgery
|
M-TEER
|
Surgery
|
M-TEER
|
Surgery
|
M-TEER
|
Surgery
|
EVEREST II,
2011
|
67.3 ± 12.8
(184)
|
65.7 ± 12.9
(95)
|
115/184
(62.5)
|
63/95
(66.3)
|
- |
- |
38/184
(20.7)*
|
18/95
(18.9)*
|
94/184
(51.1)
|
45/95
(47.4)
|
176/184
(95.7%)
|
88/95
(92.6%)
|
0.56 ± 0.38
(171)
|
0.59 ± 0.35
(87)
|
60.0 ± 10.1
(182)
|
60.6 ± 11.0
(95)
|
159.03 ± 37.33
(144)
|
160.39 ± 46.66
(66)
|
MATTERHORN,
2024
|
70.2 ± 8.1
(102)
|
70.9 ± 7.8
(101)
|
66/104
(63.5)
|
59/104
(56.7)
|
3.0
[1.6; 4.5]
(96)
|
3.0
[1.8; 4.2]
(92)
|
4/103
(3.9)*
|
3/103
(2.9)*
|
84/102
(82.4)
|
90/101
(89.1)
|
99/102
(97.1%)
|
92/97
(94.8%)
|
0.2 ± 0.1
(86)
|
0.2 ± 0.1
(76)
|
42.6 ± 10.9
(100)
|
43.4 ± 12.5
(93)
|
170.0 ± 58.2
(100)
|
158.8 ± 56.6
(93)
|
Koschutnik,
2022
|
74.0 ± 9.0
(51)
|
71.1 ± 10.1
(51)
|
18/51
(35.3)
|
22/51
(43.1)
|
6.8 ± 5.7
(51)
|
5.0 ± 3.9
(51)
|
9/51
(17.6)*
|
0/51
(0.0)*
|
44/51
(86.3)
|
39/51
(76.5)
|
- |
- |
- |
- |
52.3 ± 16.1
(51)
|
57.9 ± 13.8
(51)
|
- |
- |
Amabile,
2023
|
72.6 ± 10.1
(550)
|
72.1 ± 9.1
(550)
|
366/550
(66.6)
|
356/550
(64.7)
|
- |
- |
365/550
(66.4)
|
362/550
(65.8)
|
- |
- |
- |
- |
- |
- |
44.2 ± 16.5
(550)
|
42.3 ± 17.5
(550)
|
- |
- |
Silaschi,
2024
|
71.7 ± 8.35
(49)
|
70.0 ± 7.31
(49)
|
28/49
(57.1)
|
24/49
(49.0)
|
2.3 ± 1.39
(49)
|
1.8 ± 1.39
(49)
|
4/49
(8.2)
|
0/49
(0.0)
|
15/19
(78.9)
|
21/43
(48.8)
|
22/24
(91.7%)
|
19/23
(82.6%)
|
0.38 ± 0.21
(49)
|
0.42 ± 0.24
(49)
|
60.0 ± 8.0
(49)
|
60.5 ± 9.7
(49)
|
113.3 ± 44.9
(49)
|
125.8 ± 54.0
(49)
|
|
Pooled Total
|
71.3 ± 10.6
(936)
|
71.1 ± 9.6
(846)
|
593/938
(63.2)
|
524/849
(61.7)
|
3.83 ± 3.79
(196)∫
|
3.23 ± 2.72
(192)∫
|
420/937
(44.8)
|
383/848
(45.2)
|
237/356
(66.6)
|
195/290
(67.2)
|
297/310
(95.8)
|
199/215
(92.6)
|
0.43 ± 0.34
(306)
|
0.41 ± 0.31
(212)
|
48.4 ± 16.1
(932)
|
46.5 ± 17.4
(838)
|
155.1 ± 50.4
(293)
|
151.5 ± 54.7 (208) |
Values are expressed as mean ± standard deviation or median and [interquartile range].
CABG: coronary artery bypass graft; EROA: effective regurgitant orifice area; LVEDV: left ventricle end-diastolic volume; LVEF: left ventricle ejection fraction; MR: mitral valve regurgitation; M-TEER: mitral valve transcatheter edge-to-edge repair; NYHA: New York Heart Association. * Previous CABG only. ∫ Pooled total using estimated mean and standard deviation from median and interquartile range of MATTERHORN trial.
Significant symptomatic heart failure (NYHA class III or higher) at baseline was similarly prevalent in both groups (66.6% vs. 67.2%). Most patients had at least MR grade 3, though this was more frequent in the M-TEER group (95.8% vs. 92.6%), with slightly larger effective regurgitant orifice area (EROA) values. Mean LVEF was nearly identical (48.4 ± 16.1% vs. 46.5 ± 17.4%), while left ventricular end-diastolic volume (LVEDV) was marginally higher in the M-TEER group (155.1 ± 50.4 vs. 151.5 ± 54.7 mL).
Comorbidities were similar across groups (Supplementary Material Table 5), though coronary artery disease was more common in M-TEER patients (43.0% vs. 35.9%). Patients treated with M-TEER also demonstrated higher usage of disease-modifying therapies (Supplementary Material Table 6).
Short-Term at 30 Days Outcomes and Complications
The surgical group experienced a higher incidence of complications at 30 days compared to the M-TEER group (Table 3). This was primarily driven by a significantly greater occurrence of major bleeding (8.9% vs. 30.9%), strokes (0.6% vs. 3.0%), and new-onset atrial fibrillation (AF) (1.8% vs. 13.6%). Patients in the SMVI group also exhibited higher rates of organ failure, including prolonged mechanical ventilation (over 48 hours), deep wound infections, and renal failure requiring dialysis. Notably, the reintervention rates at 30 days were similar between the two groups (5.3% vs. 5.1%).
Table 3.
Outcomes at discharge or at 30 days
|
|
All-cause
mortality (%)
|
Reintervention (%)
|
Major bleeding (%)
|
Stroke (%)
|
New onset AF (%)
|
Myocardial infarction (%)
|
Renal failure (%)
|
Deep wound infection (%)
|
Need of mechanical ventilation>48h (%)
|
|
M-TEER
|
Surgery
|
M-TEER
|
Surgery
|
M-TEER
|
Surgery
|
M-TEER
|
Surgery
|
M-TEER
|
Surgery
|
M-TEER
|
Surgery
|
M-TEER
|
Surgery
|
M-TEER
|
Surgery
|
M-TEER
|
Surgery
|
EVEREST II,
2011 |
2/180
(1.1) |
2/94
(2.1) |
- |
1/94
(1.1) |
24/180
(13.3)* |
42/94
(44.7)* |
2/180
(1.1) |
2/94
(2.1) |
2/180
(1.1) |
0/94
(0.0) |
0/180
(0.0) |
0/94
(0.0) |
1/180
(0.6) |
0/94
(0.0) |
0/180
(0.0) |
0/94
(0.0) |
0/180
(0.0) |
4/94
(4.5) |
MATTERHORN,
2024 |
2/101
(2.0) |
4/93
(4.3) |
5/100
(5.0) |
10/91
(11.0) |
3/97
(3.1)∫ |
22/90
(24.4)∫ |
0/97
(0.0) |
4/90
(4.4) |
3/97
(3.1) |
25/90
(27.8) |
0/97
(0.0) |
1/91
(1.1) |
4/98
(4.1) |
9/92
(9.8) |
1/100
(1.0) |
4/89
(4.5) |
4/99
(4.0) |
10/92
(10.9) |
Koschutnik,
2022 |
- |
- |
3/51
(5.9) |
1/51
(2.0) |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
Amabile,
2023 |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
- |
Silaschi,
2024 |
3/49
(6.1) |
2/49
(4.1) |
- |
- |
2/49
(4.1)† |
8/49
(16.3)† |
0/49
(0.0) |
1/49
(2.0) |
- |
- |
- |
- |
1/49
(2.0) |
4/49
(8.2) |
- |
- |
- |
- |
|
Pooled Total
|
7/330
(2.1) |
8/236
(3.4) |
8/151
(5.3) |
12/236
(5.1) |
29/326
(8.9) |
72/233
(30.9) |
2/326
(0.6) |
7/233
(3.0) |
5/277
(1.8) |
25/184
(13.6) |
0/277
(0.0) |
1/185
(0.5) |
6/327
(1.8) |
13/235
(5.5) |
1/280
(0.4) |
4/183
(2.2) |
4/279
(1.4) |
14/186
(7.5) |
AF: atrial fibrillation; M-TEER: mitral valve transcatheter edge-to-edge repair; UGR: use of blood transfusion.
* Bleeding requiring 2 or more UGR
∫ Major bleeding according to Valve Academic Research Consortium (VARC)
† Bleeding Academic Research Consortium (BARC) 3 or 4
All-cause mortality at 30 days was assessed in three studies, including both RCTs (Figure 2).4,5,9 While the data indicated a trend toward higher mortality rates in the SMVI group, particularly in RCTs, no statistically significant differences were observed between the two interventions (RR: 0.72; 95% CI: 0.26–2.00).
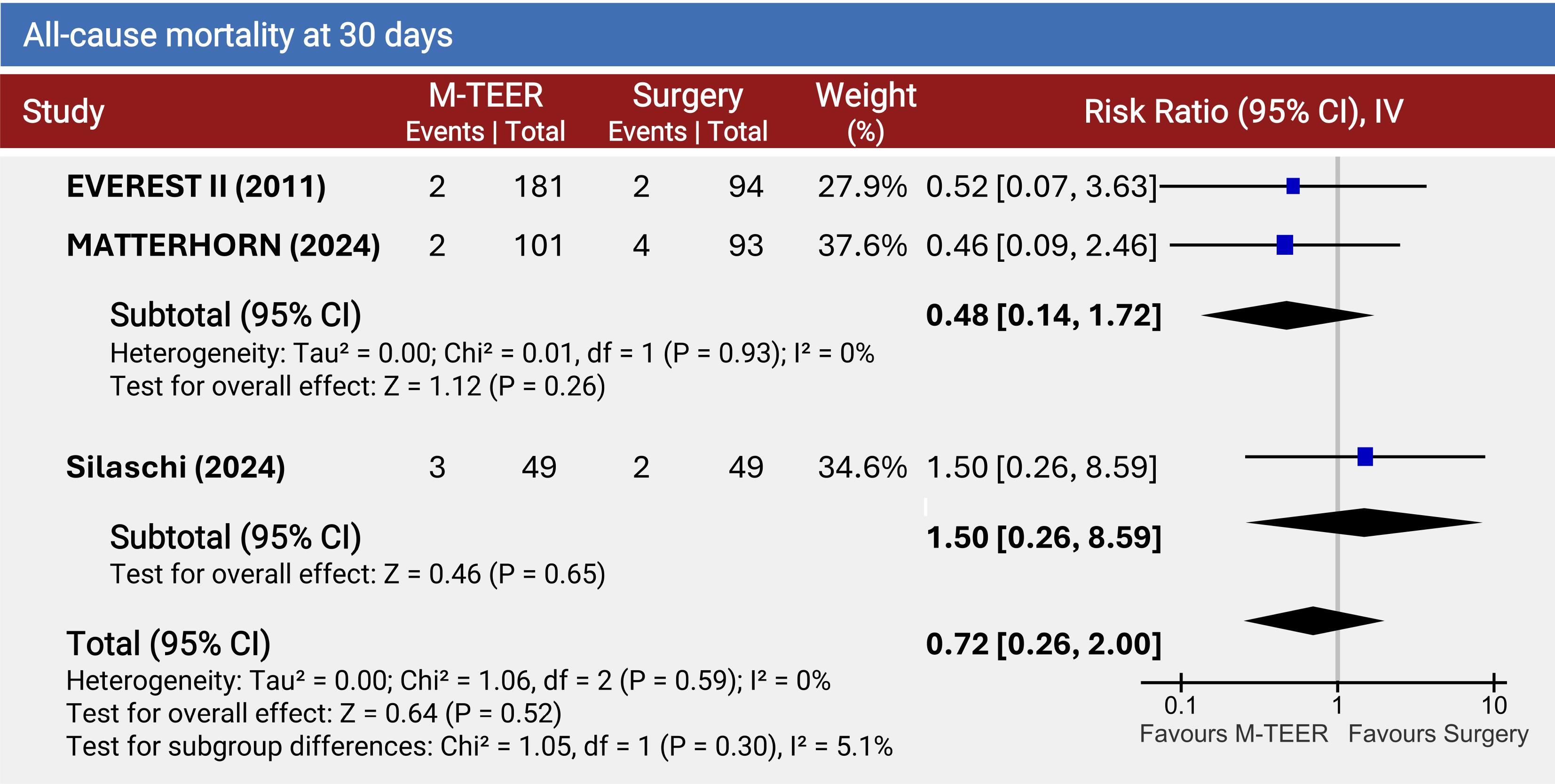
Figure 2.
Forest Plot for All-Cause Mortality at 30 Days.This forest plot compares the risk ratio (RR) of all-cause mortality at 30 days between mitral transcatheter edge-to-edge repair (M-TEER) and surgery in three studies: EVEREST II (2011), MATTERHORN (2024), and Silaschi (2024). The combined analysis shows an overall risk ratio of 0.72 (95% CI: 0.26–2.00) favoring M-TEER, though the results are not statistically significant (P = 0.52). *Only includes data from patients with primary mitral regurgitation
.
Forest Plot for All-Cause Mortality at 30 Days.This forest plot compares the risk ratio (RR) of all-cause mortality at 30 days between mitral transcatheter edge-to-edge repair (M-TEER) and surgery in three studies: EVEREST II (2011), MATTERHORN (2024), and Silaschi (2024). The combined analysis shows an overall risk ratio of 0.72 (95% CI: 0.26–2.00) favoring M-TEER, though the results are not statistically significant (P = 0.52). *Only includes data from patients with primary mitral regurgitation
Twelve-Months Follow-Up Outcomes
At 12 months (Figure 3), patients undergoing M-TEER had a significantly higher risk of all-cause mortality compared to those treated with SMVI (RR: 1.41; 95% CI: 1.11–1.81), a difference largely driven by findings from observational studies. Notably, Amabile demonstrated a significant survival benefit with SMVI at 12 months. Meanwhile, Koschutnik, which included only patients with PMR, favored surgery but without reaching statistical significance. When focusing solely on RCTs, no significant differences were observed at 12 months (RR: 0.92; 95% CI: 0.46–1.81).
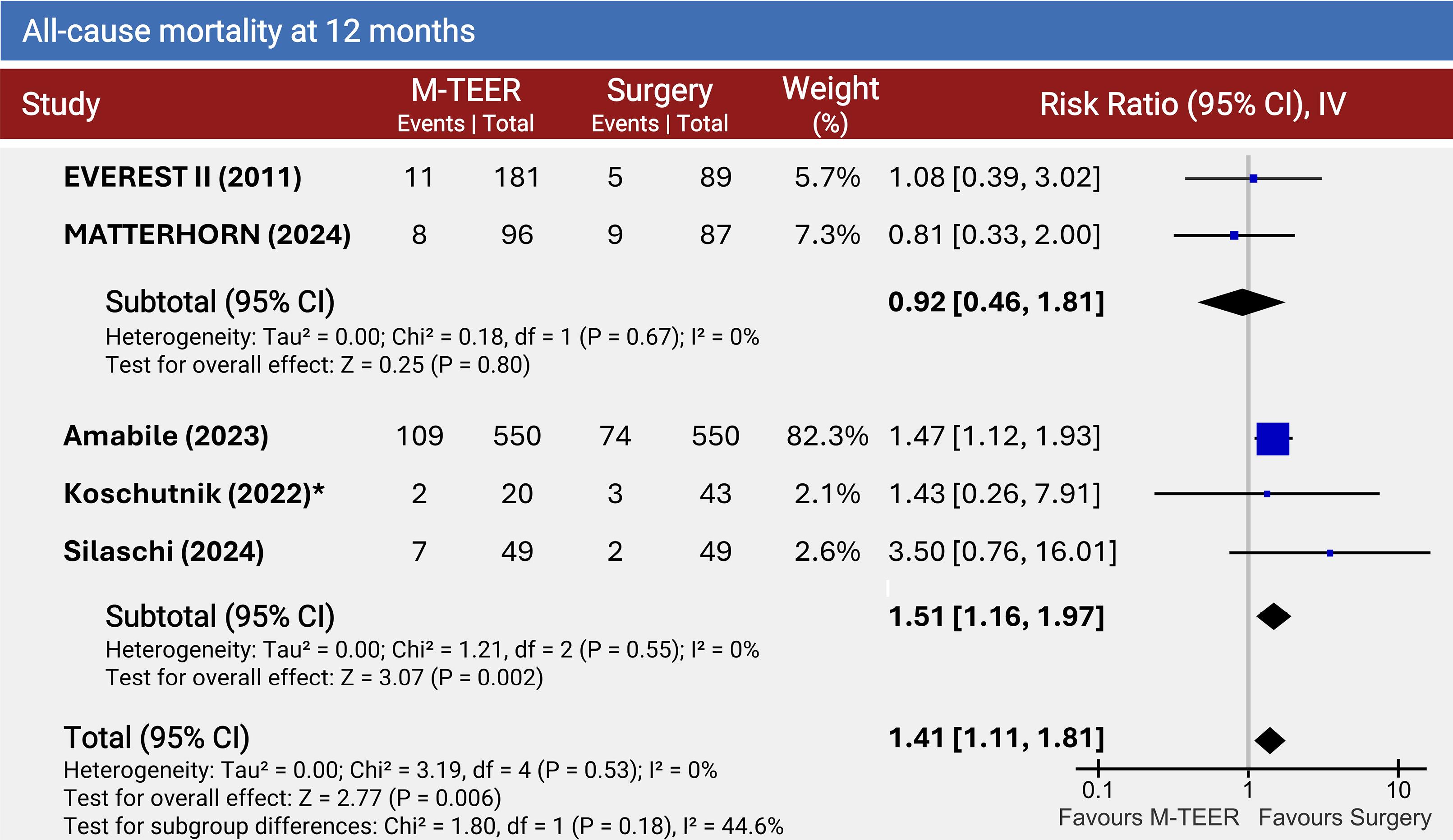
Figure 3.
Forest Plot for All-Cause Mortality at 12 months.The forest plot compares all-cause mortality between the intervention group mitral transcatheter edge-to-edge repair (M-TEER) and the surgical mitral intervention (valve repair/replacement) at 12 months across multiple studies. Risk ratios (RR) with 95% confidence intervals (CI) are presented for each study and pooled for two subgroups: randomized control trials and observational studies with propensity matched cohorts. The overall pooled analysis indicates a higher mortality risk in the M-TEER group compared to surgery (RR: 1.41, 95% CI: 1.11–1.81). *Only includes data from patients with primary mitral regurgitation
.
Forest Plot for All-Cause Mortality at 12 months.The forest plot compares all-cause mortality between the intervention group mitral transcatheter edge-to-edge repair (M-TEER) and the surgical mitral intervention (valve repair/replacement) at 12 months across multiple studies. Risk ratios (RR) with 95% confidence intervals (CI) are presented for each study and pooled for two subgroups: randomized control trials and observational studies with propensity matched cohorts. The overall pooled analysis indicates a higher mortality risk in the M-TEER group compared to surgery (RR: 1.41, 95% CI: 1.11–1.81). *Only includes data from patients with primary mitral regurgitation
The proportion of patients who did not achieve NYHA functional class I or II at 12 months was similar between the two groups, as illustrated in Figure 4A. In the EVEREST II trial, patients undergoing SMVI experienced significantly higher rates of symptomatic heart failure. However, this trend was not replicated in the MATTERHORN trial, which reported no significant differences between the groups. Conversely, the Silaschi study found that a greater proportion of patients who underwent surgery remained in NYHA functional class I or II.
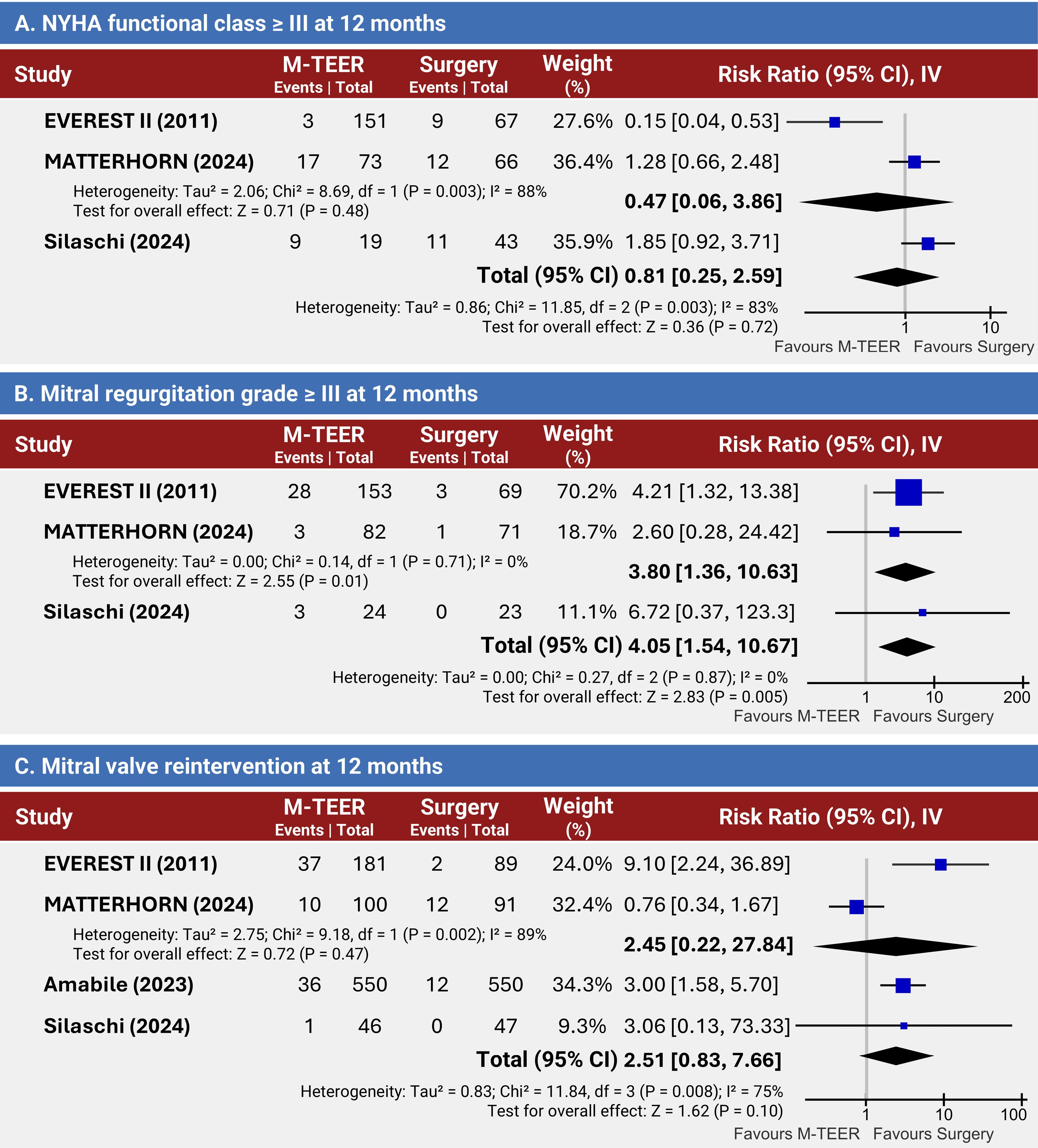
Figure 4.
Comparative Outcomes at 12 Months for M-TEER vs. Surgery.(A) Risk ratio (RR) comparing mitral transcatheter edge-to-edge repair (M-TEER) and surgery for the prevalence of NYHA functional class ≥ III at 12 months. Pooled results show no significant difference. (B) RR evaluating the persistence of mitral regurgitation (MR) grade ≥ III at 12 months. The pooled analysis indicates a higher likelihood of residual MR in patients treated with M-TEER compared to surgery. (C) RR for mitral valve reintervention at 12 months across treatment modalities. Results suggest a tendency toward higher reintervention rates in the M-TEER group compared to surgery, although no significant differences were observed in the pooled analysis.
.
Comparative Outcomes at 12 Months for M-TEER vs. Surgery.(A) Risk ratio (RR) comparing mitral transcatheter edge-to-edge repair (M-TEER) and surgery for the prevalence of NYHA functional class ≥ III at 12 months. Pooled results show no significant difference. (B) RR evaluating the persistence of mitral regurgitation (MR) grade ≥ III at 12 months. The pooled analysis indicates a higher likelihood of residual MR in patients treated with M-TEER compared to surgery. (C) RR for mitral valve reintervention at 12 months across treatment modalities. Results suggest a tendency toward higher reintervention rates in the M-TEER group compared to surgery, although no significant differences were observed in the pooled analysis.
Prevalence of MR grade 3 or higher at 12 months post-procedure was significantly higher in the M-TEER group compared to the SMVI group (RR: 4.05; 95% CI: 1.54–10.67) (Figure 4B). This finding remains unchanged when the observational study is excluded from the analysis (RR: 3.80; 95% CI: 1.36–10.63).9
At 12-month follow-up, MV reintervention rates, depicted in Figure 4C, showed no significant difference between the M-TEER and SMVI groups, although a trend favoring SMVI was noted. In the EVEREST II trial, MV reintervention was significantly more common in the M-TEER group (20.4% vs. 2.2%), a finding also observed in Amabile. In Silaschi, only one patient required reintervention.
Discussion
Over the past decade, M-TEER has emerged as a less invasive approach for patients with prohibitive surgical risk. 12-14 According to recent recommendations, M-TEER is now not only considered for patients with SMR and compromised LV function,15,16 but has also received a class IIA recommendation for treatment of PMR, as well as SMR, in the newly issued ACC/AHA guidelines.15 This upgrade in recommendation for PMR is based on registry data,17 as RCTs comparing long-term mortality outcomes between these modalities remain lacking. Given the limited randomized trial data, pooling results from these studies alongside observational studies is necessary to compare interventions effectively (Figure 5). Since M-TEER and SMVI are usually targeted at different patient populations, with M-TEER being reserved for high-risk patients who often have worse prognosis, only propensity-matched cohorts can potentially provide a robust comparison of outcomes, minimizing selection bias from clinical practice.
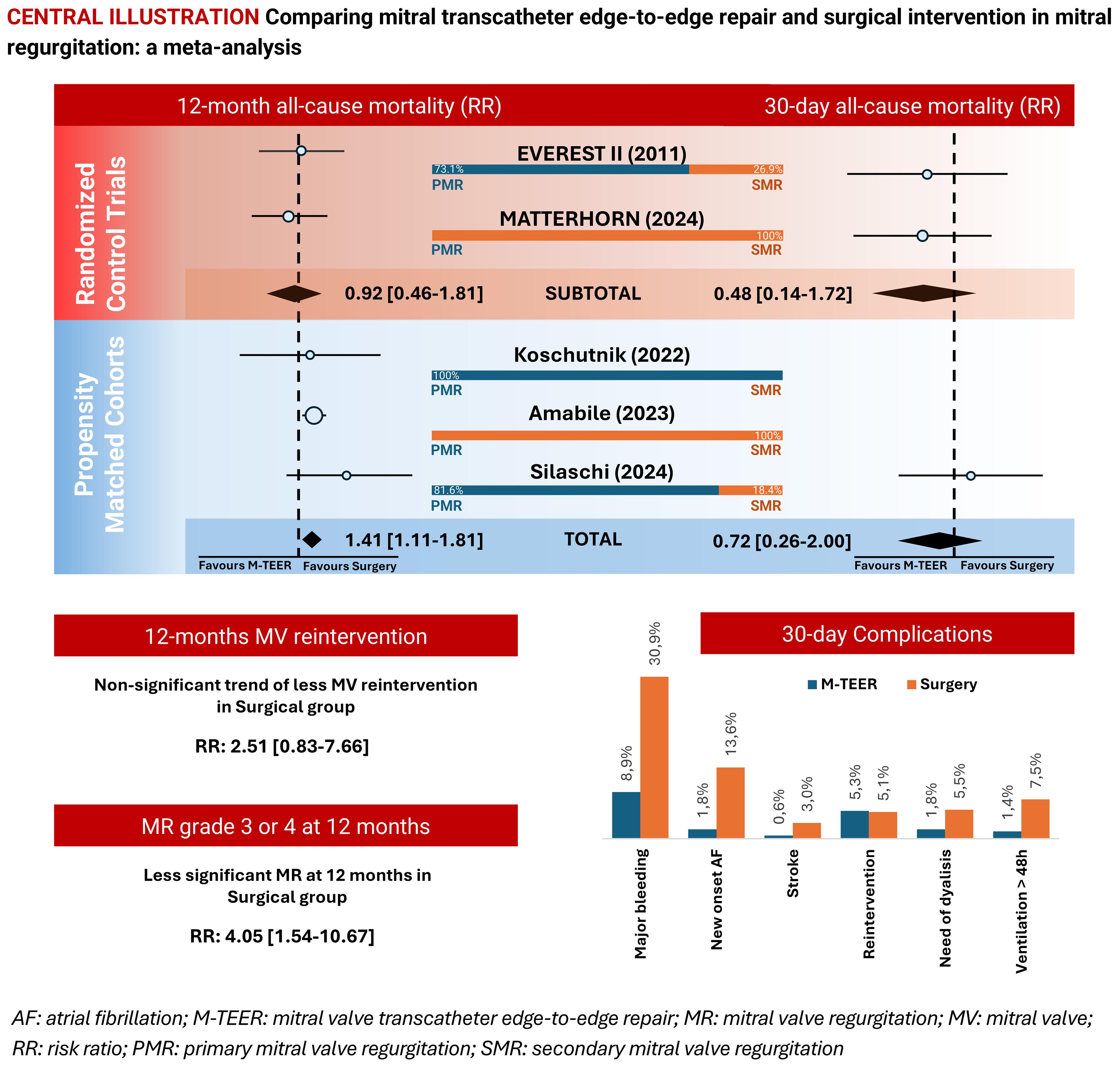
Figure 5.
Central Illustration Summarizing the Main Findings
.
Central Illustration Summarizing the Main Findings
Short-Term Outcomes
The findings highlight distinct differences in 30-day outcomes. As expected, surgery is associated with higher early complication rates, while M-TEER demonstrates fewer periprocedural adverse events and comparable reintervention rates, with a nonsignificant trend toward higher mortality in the surgical group.
The differences in complication rates were primarily driven by a higher incidence of major bleeding, stroke, and new-onset AF in the SMVI group. In fact, transfusions accounted for the largest single component of major adverse events at 30 days and have been previously linked to worse outcomes.18 In the EVEREST II trial,4 even after excluding transfusion events, the rate of adverse events remained lower in the M-TEER group, seemingly solidifying M-TEER as the better intervention in terms of short-term adverse events.
Short-term reintervention rates are not significantly different between treatment modalities, but there are differences among trials. The EVEREST II trial did not account for patients with unsuccessful M-TEER procedures who were subsequently referred for surgery in the outpatient setting, thus underestimating M-TEER rates.4 However, it is also important to note that during the EVEREST II trial, M-TEER was a novel technique with limited operator experience, resulting in higher failure rates.4 The SMVI group may have also underestimated reintervention rates, as other non-mitral valve surgery-related reinterventions in SMVI patients were not accounted for.
The suggested non-significant trend of higher mortality at 30 days in the SMVI group was primarily driven by RCT data. In contrast, the observational study may favor SMVI due to underling selection bias, even after propensity matching. In the Silaschi cohort,9 higher-risk patients may still have been more likely to be in the M-TEER group than in the SMVI group.
Twelve-Month Mortality
Our results indicated that SMVI was favored, with patients who underwent M-TEER exhibiting a significantly higher 12-month mortality risk when compared to surgical treatment. However, no comparable differences were observed when analyzing only the RCTs, with the 12-month mortality risk difference primarily driven by the observational studies.
As discussed previously, this could be due to underlying selection bias, meaning that the mortality risk may be more closely associated with the patients’ underlying conditions rather than the intervention itself. In a sensitivity analysis, exclusion of the Amabile study, which relied on ICD-10 and CPT codes and was the only purely retrospective study,11 resulted in no statistical significance observed (RR 1.18; 95% CI 0.66–2.11) (Supplementary Figure 1). Additionally, five-year mortality rates in the EVEREST II trial showed no significant difference between the groups (20.8% vs. 26.8%; P = 0.36), and treatment strategy was not associated with survival in multivariable analysis.7,8 It is also important to note that RCTs excluded patients with other severe valve disorders, such as tricuspid regurgitation, which were not excluded in the observational studies and where a considerable prevalence was observed (Supplementary Table 7).
Age and comorbidity burden naturally contribute to the pooled estimates observed. Although long-term survival in the EVEREST II trial was similar between treatment arms,4,7,8 SMR and advanced age were important predictors of decreased survival. While no meta-regression analysis was performed due to the limited data set (5 studies), the apparent impact of SMR prevalence on 12-month mortality suggests that M-TEER may provide better outcomes in patients with SMR compared to those with PMR. Whether the etiology of SMR significantly impacts the mortality effects of M-TEER and SMVI remains unknown.
These considerations highlight the complexity of interpreting trial and observational data particularly when guiding clinical decisions regarding M-TEER for patients at the threshold of surgical eligibility.
As for the comparison between M-TEER plus guideline-directed medical therapy (GDMT) and GDMT alone, it has predominantly been studied in SMR. The recently published RESHAPE-HF2 trial,19 together with data from the COAPT,20 and MITRA-FR trials,21 supports the notion that M-TEER reduces heart failure hospitalizations, as confirmed by meta-analysis.22 However, its impact on long-term mortality remains inconclusive, with pooled analyses showing only a non-significant trend toward a survival benefit.22
Functional Class, Mitral Valve Regurgitation Severity and Reintervention at 12 Months
The proportion of patients not achieving NYHA functional class I or II at 12 months was similar in both groups, though the estimated high heterogeneity due to the varied etiology prevalences across different studies and considerable follow-up loss limit the robustness of these results.
Prevalence of MR grade 3 or higher at 12 months after intervention was significantly higher in the M-TEER group, even when excluding the observational data.9 Although, it should be noted that the M-TEER group had more MR grade 3 or higher with slightly larger EROA values at baseline. The lack of annuloplasty in the percutaneous approach may also partly account for the more severe mitral regurgitation observed in the M-TEER group at 12 months.
When looking at the MATTERHORN trial,5 98.6% of patients in the surgery group had MR grade 2 or lower at 12 months of follow-up, which was better than anticipated. This difference reflects the trial’s low threshold for MV replacement rather than enforcement of surgical MV repair, which has been associated with higher recurrence rates of significant MR compared to MV replacement in other studies. The technical advances in surgical MV repair strategies and the less-advanced left ventricular disease in that cohort might also help favour surgery.
MV reintervention at 12-month follow-up showed a non-significant trend toward higher rates in the M-TEER group, favoring surgical treatment. In the EVEREST II trial,4 percutaneous treatment was associated with a markedly higher rate of additional procedures for mitral regurgitation (20.4% vs. 2.2%), a finding also observed in Amabile.11 Sensitivity analysis excluding the Amabile data demonstrated that the overall effect remained consistent (RR 2.52; 95% CI 0.37–17.15) (Supplementary Figure 2). The EVEREST II trial results may be explained by the limited experience of operators at the time of the trial.4 Notably, 28% of M-TEER patients required subsequent MV surgery, particularly within the first 6 months of follow-up. In contrast, re-intervention rates in more recent contemporary studies are much lower, as technical advancements in M-TEER, operator expertise and the development of more effective devices have greatly improved procedural success rates.23,24
Long-Term Outcomes and Durability of Mitral Valve Interventions
The long-term outcomes and durability of mitral valve interventions, particularly in the context of the EVEREST II trial, show a nuanced picture. Regarding the 5-year follow-up,7,8 despite an initial imbalance in patients with MR grade 3 or higher and a higher rate of surgery for MV dysfunction, few patients experienced worsening MR or required surgery after the 6-month follow-up threshold.
Despite SMVI demonstrating worse outcomes compared to M-TEER in the first 30 days, SMVI seems to be a better option in terms of reintervention and MR recurrence at 12 months, as most reinterventions resulting from insufficient MR reduction in M-TEER occur within the first 6 months. This trend reflects the nature of clinical failures associated with M-TEER observed in the EVEREST II trial, where most failures occur within the first six months, primarily due to insufficient MR reduction during the initial procedure or early complications. After this period, there was no significant difference in MR occurrence or the need for MV reintervention between the 1-year and 4-year follow-up periods,7,8 nor was there differences in mortality or decline in LV systolic function beyond 12 months, despite the higher prevalence of severe residual MR in the M-TEER group at 1 year.7,8 These observations linked to the sustained reduction in symptoms and left ventricular dimensions at 5 years,7,8 counter concerns that greater residual MR 6 months after successful M-TEER leads to reduced long-term survival. The clinical course after the initial 6-month window provides reassurance that early complications or insufficient MR reduction do not necessarily translate into long-term mortality or functional decline.
Nevertheless, extended follow-up results from the MATTERHORN trial are anticipated to provide additional data to corroborate these findings, as the EVEREST II trial remains the only study with long-term follow-up to date.
Several limitations should be acknowledged when interpreting our findings. The clinical trials included in this analysis were conducted at different times, which influenced the experience of operators and the available disease-modifying therapies. Additionally, the varying patient populations and etiologies across these trials limit the external validity of pooled results.
Observational studies inherently lack randomization, which means certain variables, some of which may not even be identified, are not randomized and can impact the results. While a propensity-matched cohort strategy was employed to minimize the expected heterogeneity of the sample, considerable differences may remain. It is important to note that while surgical risk was used for propensity matching, this risk estimate has not been as reliable for MV repair surgery as it has been for aortic stenosis interventions.25 MV repair typically has low operative mortality rates and often uses minimally invasive techniques that contribute to quicker post-operative recovery.15
Significant heterogeneity exists in the patient populations across studies. There are considerable differences in the proportions of MR etiologies among the studies. The M-TEER group had a higher Euro-Score II surgical risk and greater prevalence of coronary artery disease. Additionally, more severe MR was observed in the M-TEER group, along with slightly larger EROA values and marginally higher LVEDV values. The use of different techniques in the comparator groups may further contribute to the heterogeneity of the pooled population, potentially influencing the results and effect estimates. Given this variability, a random-effects model was selected for meta-analytic pooling to account for anticipated differences in treatment effects across studies, rather than assuming a single common effect size as in fixed-effects models. This approach allowed each study to estimate a different, yet related, underlying effect, making it more appropriate in the context of clinical and methodological heterogeneity. It also supported a more conservative and potentially more generalizable interpretation of the findings, particularly when synthesizing evidence from both randomized trials and observational studies. The reliance on study-level summary data further limits the ability to adjust for confounding factors or perform subgroup analyses, thereby restricting cross-trial comparisons.
Our studies’ endpoint is restricted to 1 year which may be too short to fully appreciate the benefits of surgery when comparing with M-TEER. Extended results from the MATTERHORN trial will certainly add valuable information to the field.
Conclusion
In conclusion, a non-significant trend of higher mortality at 30 days was observed in the SMVI group, due to higher complication rates due to bleeding. At 12 months follow-up, SMVI was associated with a significantly lower risk of all-cause mortality, while the M-TEER group had more severe residual MR, with a non-significant trend of higher rate of MR reintervention.
Based on current evidence, M-TEER should continue to be reserved for patients with prohibitive high surgical risk. While propensity-matched cohorts were pooled for the study estimates, the limited available data from randomized trials, combined with heterogeneity in patient populations, particularly regarding MR etiology, underscores the need for further studies.
Competing Interests
No conflicts of interest to declare.
Ethical Approval
As this study is a systematic review and meta-analysis, it did not involve direct interaction with human participants or animals, and therefore, no ethical approval or informed consent was required. However, the study adheres to the ethical conduct policy outlined by the International Committee of Medical Journal Editors (ICMJE) (http://www.icmje.org/).
Supplementary Files
Supplementary file 1 contains Tables S1-S7 and Figures S1-S2.
(pdf)
References
- Douedi S, Douedi H. Mitral regurgitation. In: StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing; 2024. Available from: https://www.ncbi.nlm.nih.gov/books/NBK553135/.
- Gummert JF, Funkat AK, Beckmann A, Ernst M, Hekmat K, Beyersdorf F. Cardiac surgery in Germany during 2010: a report on behalf of the German Society for Thoracic and Cardiovascular Surgery. Thorac Cardiovasc Surg 2011; 59(5):259-67. doi: 10.1055/s-0030-1271191 [Crossref] [ Google Scholar]
- Patel JB, Borgeson DD, Barnes ME, Rihal CS, Daly RC, Redfield MM. Mitral regurgitation in patients with advanced systolic heart failure. J Card Fail 2004; 10(4):285-91. doi: 10.1016/j.cardfail.2003.12.006 [Crossref] [ Google Scholar]
- Feldman T, Foster E, Glower DD, Kar S, Rinaldi MJ, Fail PS. Percutaneous repair or surgery for mitral regurgitation. N Engl J Med 2011; 364(15):1395-406. doi: 10.1056/NEJMoa1009355 [Crossref] [ Google Scholar]
- Baldus S, Doenst T, Pfister R, Gummert J, Kessler M, Boekstegers P. Transcatheter repair versus mitral-valve surgery for secondary mitral regurgitation. N Engl J Med 2024; 391(19):1787-98. doi: 10.1056/NEJMoa2408739 [Crossref] [ Google Scholar]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021; 372:n71. doi: 10.1136/bmj.n71 [Crossref] [ Google Scholar]
- Feldman T, Kar S, Elmariah S, Smart SC, Trento A, Siegel RJ. Randomized comparison of percutaneous repair and surgery for mitral regurgitation: 5-year results of EVEREST II. J Am Coll Cardiol 2015; 66(25):2844-54. doi: 10.1016/j.jacc.2015.10.018 [Crossref] [ Google Scholar]
- Mauri L, Foster E, Glower DD, Apruzzese P, Massaro JM, Herrmann HC. 4-year results of a randomized controlled trial of percutaneous repair versus surgery for mitral regurgitation. J Am Coll Cardiol 2013; 62(4):317-28. doi: 10.1016/j.jacc.2013.04.030 [Crossref] [ Google Scholar]
- Silaschi M, Cattelaens F, Alirezaei H, Vogelhuber J, Sommer S, Sugiura A. Transcatheter edge-to-edge mitral valve repair versus minimally invasive mitral valve surgery: an observational study. J Clin Med 2024; 13(5):1372. doi: 10.3390/jcm13051372 [Crossref] [ Google Scholar]
- Koschutnik M, Dannenberg V, Donà C, Nitsche C, Kammerlander AA, Koschatko S. Transcatheter versus surgical valve repair in patients with severe mitral regurgitation. J Pers Med 2022; 12(1):90. doi: 10.3390/jpm12010090 [Crossref] [ Google Scholar]
- Amabile A, Muncan B, Geirsson A, Kalogeropoulos AP, Krane M. Surgical versus interventional mitral valve repair: analysis of 1,100 propensity score-matched patients. Journal of Cardiac Surgery 2023; 2023(1):8838005. doi: 10.1155/2023/8838005 [Crossref] [ Google Scholar]
- McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J 2021; 42(36):3599-726. doi: 10.1093/eurheartj/ehab368 [Crossref] [ Google Scholar]
- Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP 3rd, Guyton RA. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014; 129(23):2440-92. doi: 10.1161/cir.0000000000000029 [Crossref] [ Google Scholar]
- Baumgartner H, Falk V, Bax JJ, De Bonis M, Hamm C, Holm PJ. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J 2017; 38(36):2739-91. doi: 10.1093/eurheartj/ehx391 [Crossref] [ Google Scholar]
- Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP 3rd, Gentile F. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021; 143(5):e35-71. doi: 10.1161/cir.0000000000000932 [Crossref] [ Google Scholar]
- Stone GW, Lindenfeld J, Abraham WT, Kar S, Lim DS, Mishell JM. Transcatheter mitral-valve repair in patients with heart failure. N Engl J Med 2018; 379(24):2307-18. doi: 10.1056/NEJMoa1806640 [Crossref] [ Google Scholar]
- Sorajja P, Vemulapalli S, Feldman T, Mack M, Holmes DR Jr, Stebbins A. Outcomes with transcatheter mitral valve repair in the United States: an STS/ACC TVT registry report. J Am Coll Cardiol 2017; 70(19):2315-27. doi: 10.1016/j.jacc.2017.09.015 [Crossref] [ Google Scholar]
- Murphy GJ, Reeves BC, Rogers CA, Rizvi SI, Culliford L, Angelini GD. Increased mortality, postoperative morbidity, and cost after red blood cell transfusion in patients having cardiac surgery. Circulation 2007; 116(22):2544-52. doi: 10.1161/circulationaha.107.698977 [Crossref] [ Google Scholar]
- Anker SD, Friede T, von Bardeleben RS, Butler J, Khan MS, Diek M. Transcatheter valve repair in heart failure with moderate to severe mitral regurgitation. N Engl J Med 2024; 391(19):1799-809. doi: 10.1056/NEJMoa2314328 [Crossref] [ Google Scholar]
- Haddadi H, Asham O, Soleimani A. Evaluation of risk factors in patients with calcific aortic valve disease who underwent aortic valve replacement from 2011 to 2021. Biomed Advances 2025; 2(1):45-9. doi: 10.34172/bma.14 [Crossref] [ Google Scholar]
- Obadia JF, Messika-Zeitoun D, Leurent G, Iung B, Bonnet G, Piriou N. Percutaneous repair or medical treatment for secondary mitral regurgitation. N Engl J Med 2018; 379(24):2297-306. doi: 10.1056/NEJMoa1805374 [Crossref] [ Google Scholar]
- Anker MS, Porthun J, Bonnet G, Schulze PC, Rassaf T, Landmesser U. Percutaneous transcatheter edge-to-edge repair for functional mitral regurgitation in heart failure: a meta-analysis of 3 randomized controlled trials. J Am Coll Cardiol 2024; 84(24):2364-8. doi: 10.1016/j.jacc.2024.08.026 [Crossref] [ Google Scholar]
- Praz F, Braun D, Unterhuber M, Spirito A, Orban M, Brugger N. Edge-to-edge mitral valve repair with extended clip arms: early experience from a multicenter observational study. JACC Cardiovasc Interv 2019; 12(14):1356-65. doi: 10.1016/j.jcin.2019.03.023 [Crossref] [ Google Scholar]
- Lim DS, Kar S, Spargias K, Kipperman RM, O’Neill WW, Ng MK. Transcatheter valve repair for patients with mitral regurgitation: 30-day results of the CLASP study. JACC Cardiovasc Interv 2019; 12(14):1369-78. doi: 10.1016/j.jcin.2019.04.034 [Crossref] [ Google Scholar]
- Carino D, Denti P, Ascione G, Del Forno B, Lapenna E, Ruggeri S. Is the EuroSCORE II reliable in surgical mitral valve repair? A single-centre validation study. Eur J Cardiothorac Surg 2021; 59(4):863-8. doi: 10.1093/ejcts/ezaa403 [Crossref] [ Google Scholar]